Perimenopause
Perimenopause means the time of life before menopause where there is lots of hormonal flux and brain vulnerability. Traditionally perimenopause was defined as lasting 2-5 years and based on changes in the menstrual cycle (eg length and change of flow). However, for many women the mood changes occur prior to the physical symptoms of menstrual change and hot flushes. Therefore perimenopause can easily last 10-12 years, and begin in the late 30s, with out any medical cause for concern. However, for some women debilitating psychological (eg anxiety) and physical (eg migraine, body pains) can occur in the perimenopause.

About Perimenopause
Learn more through our Insights and Popular Updates

MEDICATION: Estradiol
MEDICATION: Progesterone in Peri
WEBINAR: Perimenopause

INVESTIGATION: USS

SYMPTOM: Abnormal uterine bleeding

LISTEN: ADHD and hormones

MEDICATION: Utrogestan

VIDEO: Vaginal progesterone
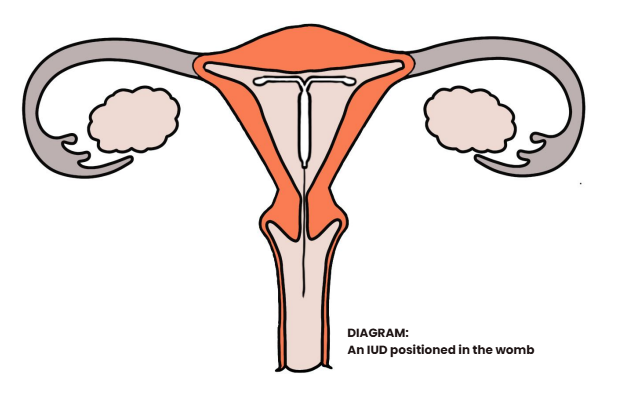
MEDICATION: Mirena
SYMPTOM: Migraine

MANANGE: Menstrual Migraines

MANAGEMENT: Dry skin

SYMPTOM: Itchy skin

Autism + Menopause

LEARN: Alcohol and Menopause

LEARN: Estrogen
LEARN: Am in in Perimenopause?

MEDICATION: Blocking your hormones

PCOS: More than just irregular periods

MEDICATION: Slinda (Drosperinone 4mg)

MEDICATION: Depot & Perimenopause
SYMPTOM: I am not feeling myself

Sensitive to hormones? Try responsive..